
Dani is a 29 year parturient, G1P0, at 36 weeks gestation with a diagnosis of Hodgkins Disease since 17 weeks gestation.
She has been admitted to your hospital's obstetric unit with a 24 hour history of general malaise, fever and reduced foetal movements. There is no history of infectious contacts or recent travel.
Past Medical History
Stage IV Hodgkins Disease (Nodular Lymphocyte predominant Hodgkins Lymphoma)
- Treated with 6 cycles R-CHOP
- Last dose of treatment: Rituximab only, 7 days ago.
Obesity (BMI 45)
OPENING QUESTION
Candidate has 2 minutes reading time to plan their initial response to the first question below
Click each question to reveal a suggested answer
Explain what Hodgkins Disease is, and how you assess the severity of Dani’s disease?
Type of lymphoid malignancy that primarily affects the lymph nodes. Patients typically present with painless enlarged lymph nodes and general systemic symptoms including malaise, fever, night sweats and unexplained weight loss.
Markers of Severity
B-symptoms: fever > 38, sweats, weight loss > 10% in 6 months
Large mediastinal mass / lymphadenopathy
Stage of disease (I - IV)
> 3 - 4 sites of involvement
Extranodal disease
Information for the Candidate:
She gives a history of increasing back pain and bilateral thigh pain intermittently over the last 2 weeks. On a neurological exam her lower limb power and sensation are normal. Her Perineal sensation is intact.
On airway assessment, she has Mallampati 2, short neck and pain on neck extension with reduced range. She gets shooting electric pain down both upper arms when she lifts her head up.
Oncology has been consulted and a whole body MRI is ordered.
PROGRESS QUESTIONS
Comment on this MRI report (click to read)
Large mass centred at L4, causing central canal stenosis and compressing the thecal sac and cauda equina towards the right. There is likely compression of the left L3 and bilateral L4 exiting nerves. There is also diffuse osseous involvement of the visualised vertebra. At the cervical spine there is mild cord compression at C4 and C5 from tumour and osseous destruction at the same level.
This is likely in keeping with epidural lymphoma with multi spinal level involvement. It is crucial to document baseline neurological function. Neuraxial techniques for labour analgesia / LSCS will likely be contraindicated.
DDx: epidural abscess, haematoma
Describe your unique anaesthetic considerations for this condition?
This patient presents with a rare and complex overlap of oncological, obstetric, and neurological comorbidities. Key anaesthetic considerations include: 1. Neurological Status and Spinal Pathology Epidural lymphoma at L4, with compression of the thecal sac and cauda equina, increases risk of worsening neurological injury with neuraxial techniques. Risk of tumour vascularity, unpredictable spread of local anaesthetic, or trauma to compromised cord or nerve roots. General anaesthesia must be a considered modality 2. Systemic effects of R-CHOP Chemotherapy Rituximab → infusion reactions, prolonged B-cell depletion (infection risk). Cyclophosphamide → potential cardiomyopathy (needs echo). Hydrodoxorubicin (Doxorubicin) → potential cardiomyopathy (needs echo). Oncovin (Vincristine) neurotoxicity → baseline neuropathy. Prednisone → immunosuppression 3. Residual Tumour Burden New MRI - signficant tumour Compression effects may evolve, especially with pregnancy-related fluid shifts and raised IAP. 4. Obesity (BMI 37) Difficult airway, IV access, positioning, higher risk of aspiration and DVT. Increased technical difficulty for neuraxial techniques. 5. Peripartum Planning Will require coordinated MDT delivery plan at a tertiary centre: oncology, MFM, anaesthesia, neonatology. Timing of delivery (balancing maternal disease progression vs foetal maturity). 6. Trauma Informed Care and Patient Psychological Vulnerability Pre-existing anxiety and depression in setting of Stage IV cancer. This context demands compassionate, clear counselling and patient-centred decision making.
What investigations would you want prior to delivery?
To ensure safe peripartum management, I would review / perform:
1. Neurological
Repeat MRI of spine to assess for interval change or worsening compression. Ideally within 2–3 weeks of planned delivery.
Perform a baseline neurological exam and document
2. Cardiac
ECG & Echocardiogram: Assess for anthracycline (doxorubicin)-induced cardiomyopathy.
3. Infectious Screen
FBC, neutrophil count: assess for immunosuppression, particularly neutropaenia
Would you consider regional anaesthesia for her delivery? Why or why not?
Neuraxial anaesthesia is not safe in this case due to:
Against Regional:
Known epidural tumour with spinal canal stenosis and compression of the thecal sac.
Unpredictable spread of local anaesthetic (due to mass effect, distorted anatomy).
Risk of direct trauma or bleeding into tumour.
Potentially cause a new neurological deficit.
In Favour of Regional (Very Conditional):
If updated MRI shows resolution or significant regression of epidural disease.
If no current neurological signs and MRI shows safe zone in lumbosacral spine.
Only under expert hands, and ideally at a level not involved with tumour.
Conclusion:
In the current context, neuraxial techniques are contraindicated. The patient can only have a GA for LSCS and non-neuraxial analgesia techniques for labour.
3 days later the patient develops PPROM (preterm premature rupture of membranes). She has mild abdominal cramps but not in active labour. The Obstetrics team have consented her for a LSCS just in case. She is anxious and strongly wants to avoid GA. How do you approach this?
This is a high-stakes shared decision-making scenario requiring empathy and clarity.
1. Acknowledge Concerns and Rebuild Trust
Validate her fears of general anaesthesia.
Explain your rationale clearly, using lay terms.
2. Explain the Risks of Neuraxial Anaesthesia
Outline risk of permanent neurological injury due to known tumour at L4.
Discuss unpredictability of block, potential for inadequate analgesia, or harm.
3. Present a Plan That Incorporates Her Wishes Safely
Offer labour analgesia with remifentanil PCA if appropriate and monitored.
4. Prepare for General Anaesthesia if Required
Reassure that GA can be done safely with experienced staff and preparation.
Preoxygenation, modified RSI, second airway plan, minimise aspiration risk.
5. Document and Debrief
Record the shared decision-making process.
Offer follow-up and counselling postnatally, especially if birth experience is distressing.
CHALLENGE QUESTIONS
Over the next 6 hours she has frequent episodes of unprovoked decels on CTG and foetal bradycardia (as low as 60bpm) that improves within 2 – 3min with position changes. Foetus does not tolerate maternal supine position. The Obstetrician books her for a Cat 1 LSCS for foetal distress. What is your plan for anaesthesia?
In this setting, time is limited but not “crash” — prioritise safety and efficiency.
General Anaesthesia + Post-op TAP blocks
Preparation:
Video laryngoscope / Difficult airway trolley available.
Preoxygenation and aspiration prophylaxis (sodium citrate).
Ongoing CTG monitoring until induction and parallel intrauterine resuscitation
Induction:
Modified RSI with suxamethonium / rocuronium & adjuncts
May need left uterine displacement / left lateral title during induction - for foetal resus and preventing haemodynamic compromise to patient.
If candidate does not offer, query what induction agents they intend to use - specifically propofol vs thiopentone and what opioids if any.
Intraoperative:
Careful positioning: ramped, leg support,
Avoid neck manipulation, use hyperangulated VL
Multimodal analgesia plan: IV opioids, paracetamol +/- ketamine +/- TAP blocks.
Fluid management judicious — avoid overload.
Post-op:
Monitor for respiratory depression or delayed emergence.
Early Oncology review to strategise tumour reassessment (MRI or PET) early postpartum.
The midwifery team continue CTG monitoring as you prepare on the table. At the last moment the abdomen is prepared with sterile disinfectant and draped. You induce the patient with anaesthesia as you described and proceed to intubate the patient. This is the view you achieve (click here for image). Comment on this laryngoscopy.

If VL: POGO 0%
If DL: Grade 4 (Cormack-Lehane)
What is your immediate priority and your next steps?
Immediate priority is to maintain oxygenation - there is a high risk of rapid desaturation
Verbalise to the OT team I have a difficult intubation
Re-establish gentle bag-mask ventilation (ensuring PIP < 20 cmH2O to avoid overinflating the stomach)
(and continuing apnoeic oxygenation via HFNP if used)
The candidate can have multiple correct responses of specific management in acheiving a secure airway. The key is having a logical stepwise strategy in dealing with this specific situation.
Examples (will depend on initial response):
- Optimise intubating conditions: remove cricoid pressure, external laryngeal manipulation, reposition head and neck (need to recognise this will be limited due to pathology), use bougie / stylet
- Call for help from senior colleague to standby if 2nd attempt fails.
- Proceed with 2nd attempt: consider using alternate VL or advanced technique e.g. fibreoptic bronchoscope
You cannot ventilate effectively with the facemask and proceed to the second attempt at laryngoscopy the view is only marginally improved. Your intubation fails again. The foetal bradycardia has not resolved. There is no other anaesthetist available. The patient vital signs: HR 125, BP 113/80, SpO2 91%, (FiO2 100%). What do you do?
Given multiple failed intubations and higher risk of escalating to a "cannot intubate/cannot oxygenate" (CICO) situation, where airway swelling can develop very rapidly, I would choose to secure the airway immediately with a second-generation supraglottic airway.
The priority is to establish and maintain oxygenation. A second-generation SAD is a safe and rapidly deployable rescue airway. If it provides effective oxygenation and ventilation it can also prevent the need for FONA.
I recognise however the relative higher risk of aspiration in the parturient but this must be balanced by the risk of maternal / neonatal hypoxia and death.
Aspiration can be partly mitigated even with an SAD by suctioning a gastric tube passed through the SAD and minimizing fundal pressure at delivery.
(The OAA/DAS guidelines).
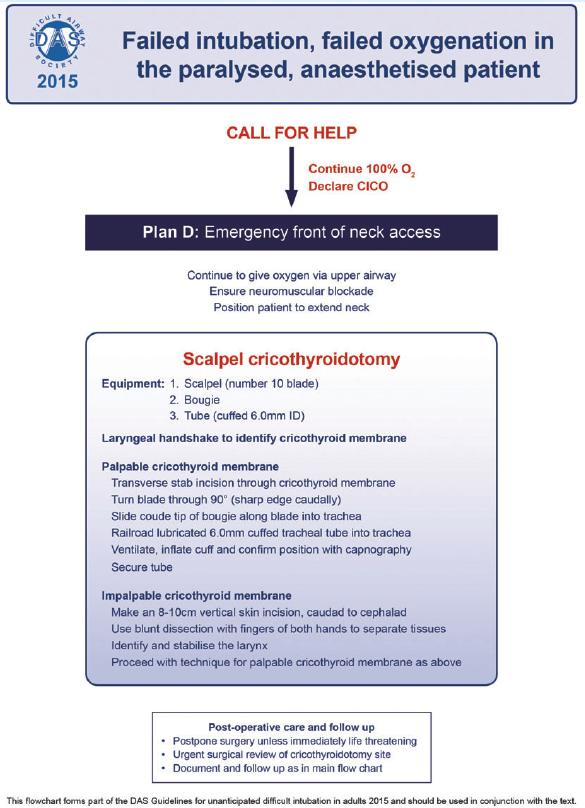
The LMA is inserted. SpO2 is now 82%. When you squeeze the ventilation bag it collapses easily. The chest does not rise. There is no capnography observed. What is your next steps?
This is an airway crisis. A CICO situation. Consequently failed facemask ventilation, intubation and LMA.
This MUST be recognised and the management must be sound. This is a pass/fail point.
Extend the head and neck to optimise FONA
Use scalpel bougie / needle cricothyroidotomy technique
- must be described accurately and succintly.
- waveform capnography must be part of confirmation of tracheal placement.
- if needle technique, must also convert to an ETT (e.g. using Melker kit)
e.g.
AFTERMATH QUESTIONS
The FONA is successful. You tell the obstetrician to proceed and the neonate is delivered within 5min. The paediatrician resuscitates the baby with CPAP but is otherwise well. The rest of the surgery is uneventful. What is your post-op care of this patient?
Immediate
Maintain anaesthesia / sedation
Ensure airway secure
Optimise analgesia: lateral TAP blocks +/- PCA
Oxytocin infusion: 10units/hour
Post-OT
ICU admission
Referral to ENT for consideration of formal tracheostomy
Documentation
Internal incident report logs / WEBAIRS
Debriefs
Communication with NOK
Register difficult intubation with and alert card / letters sent to the patient, GP and hospital alert system
M&M
END OF VIVA
Sources
Kieron Dunleavy, Claire McLintock; How I treat lymphoma in pregnancy. Blood 2020; 136 (19): 2118–2124. doi: https://doi.org/10.1182/blood.2019000961
LaCasce AS, Ng AK. Pretreatment evaluation, staging, and treatment stratification of classic Hodgkin lymphoma. UpToDate 2024. https://www.uptodate.com.acs.hcn.com.au/contents/pretreatment-evaluation-staging-and-treatment-stratification-of-classic-hodgkin-lymphoma?search=hodgkin%20lymphoma§ionRank=1&usage_type=default&anchor=H2&source=machineLearning&selectedTitle=3~150&display_rank=3#H3262774990
Ng AK, Aster JC, Herrera AF. Classic Hodgkin lymphoma: Presentation, evaluation, and diagnosis in adults. UpToDate 2024. https://www.uptodate.com.acs.hcn.com.au/contents/classic-hodgkin-lymphoma-presentation-evaluation-and-diagnosis-in-adults?search=hodgkin%20lymphoma&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1
Odor, P.M., Bampoe, S., Moonesinghe, S.R., Andrade, J., Pandit, J.J., Lucas, D.N. and Pan-London Perioperative Audit and Research Network (PLAN), for the DREAMY Investigators Group (2021), General anaesthetic and airway management practice for obstetric surgery in England: a prospective, multicentre observational study*. Anaesthesia, 76: 460-471. https://doi.org/10.1111/anae.15250
Delgado C, Ring L, Mushambi MC. General anaesthesia in obstetrics. BJA Education, 20(6): 201e207 (2020). https://doi: 10.1016/j.bjae.2020.03.003
T.M. Price & E.P. McCoy. Emergency front of neck access in airway management. BJA Education, 19(8): 246e253 (2019). https://doi: 10.1016/j.bjae.2019.04.002
Whatling E, Jones C, Chrisman L. Adult front of neck airway: a narrative review. J Oral Maxillofac Anesth 2024;3:22 | https://dx.doi.org/10.21037/j
