
Olivia is a 29 year old pregnant woman at 27 weeks gestation, G2 P1. Her obstetric team has referred her to pre-admission clinic because of her complex medical background. She recently had an admission to hospital for hyperglycaemia and pancreatitis during this antenatal period. Her past medical history includes:
Type 2 diabetes mellitus
Retinopathy
Pedal neuropathy
Chronic hypertension
Chronic tachycardia
Obesity (Class 3, BMI 45, 127kg)
Chronic pancreatitis
Asthma
Polycystic ovarian syndrome
Depression and anxiety
DVT - right arm
Medications:
Insulin Lispro (Humalog) 100 IU TDS
Insulin Detemir (Levemir) 95 IU mane, 20IU nocte
Metformin 500mg BD
Sertraline 150mg OD
Esomeprazole 80mg BD
Fenefibrate 145mg OD
Verapamil 180mg OD
Atorvastatin 20mg OD
Aspirin 150mg OD
Folic acid 5mg
Elevit
Allergies:
Morphine
Suxamethonium
Latex
OPENING QUESTION
Candidate has 2 minutes reading time to plan their initial response to the first question below
Click each question to reveal a suggested answer
What further information would you seek?
Given the high complexity of this patient - an opening statement recognising this challenge is useful: "Olivia represents an exceptionally high-risk obstetric patient with complex multisystem comorbidities. She will require a MDT approach to minimise her perinatal risk"
In addition to my usual anaesthetic assessment, the focus of my review is to determine the severity and stability of these key issues through history, exam, investigations and patient's old medical records:
- Endocrine and metabolic
- Evidence of microvascular disease raises concern of macrovascular complications from T2DM given her CVS risk factor profile of severe obesity, hypertension and thrombosis.
- Quantify with HBA1c and recommend a BSL diary for the duration of pregnany
- Any recent insulin or OHA escalations in dosing or introduction of new agents?
- History of acute poor BSL control e.g. ketoacidosis, HONK or hypo/hyper-glycaemia?
- management of pancreatitis
- Cardiac
- symptoms of IHD or failure – angina, SOBOE?
- exercise tolerance before pregnancy and now?
- can use DASI to objectively measure
- Respiratory
- asthma – frequency of exacerbations, hospital presentations and ICU admissions, recent increase use of relievers/bronchodilators
- previous PEFR records and trends
- symptoms of OSA and risk profile according to STOPBANG score
- Thrombotic risk
- Context of the arm DVT – provoked vs unprovoked? During pregnancy?
- Notaby greater risk with pregnancy and co-morbidities
- Is the aspirin for VTE or other indication, noting aspirin is generally not suitable for anticoagulation
- Allergies to morphine and suxamethonium
- context? reactions – was there anaphylaxis to sux, what happens to morphine? formal testing / allergy clinic?
- Review old anaesthetic records for unusual events related to adverse drug reactions and intubation grade
- Obstetric history
- In first pregnany, what were the antenatal issues previously and mode of delivery? Any neuraxial from last time?
- Any antenatal conditions e.g. pre-eclampsia, VTE, thrombocytopaenia
PROGRESS QUESTIONS
On your assessment Olivia reports multiple hospital admissions during this pregnancy for hyperglycaemia, migraines and recurrent pancreatitis.
She had a spike in BSL up to 25 mmol/L on a routine antenatal check and her Endocrinologist increased her Humalog from 80 TDS to 100 TDS.
Her migraines have increased in frequency and she manages with paracetamol, oxycodone.
She was admitted early in the year for pancreatitis, associated with severe pain requiring hydromorphone PCA and ketamine infusion.
Prior to that she had thrombophlebitis from a PICC line she had for recurrent pilonidal MRSA abscess. She stresses that she is difficult to cannulate and often requires PICC lines during hospital admissions.
GAs in 4 – 5 years ago were uneventful – both grade 1 intubations with C-MAC size 3 videolaryngoscope electively used. Easy BVM ventilation with no Guedel.
Epidural for previous pregnancy 6 years ago. It required multiple attempts due to her scoliosis. Once it was established it worked really well for labour. Her delivery was escalated to an emergency LSCS for failure to progress. It was complicated with pre-eclampsia and post-op wound dehiscence. A labetalol infusion was required.
Given this extra information, what investigations will you seek, if any (click here for answer)?
(Rationale should be given for investigations) Review / order / perform recent:
- FBC – for anaemia and thrombocytopaenia
- UEC – for baseline renal function
- HBA1c – poorly controlled diabetes and chronic pancreas dysfunction
- ECG – baseline rhythm given multiple cardiovascular risk factors
- Foetal US for any abnormal placenta implantation – increased risk of APH / PPH
- Bedside US of lumbar spine given risk factors for difficult neuraxial block
Test results (click here to reveal):
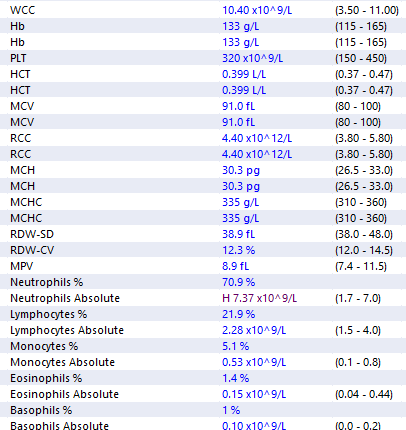
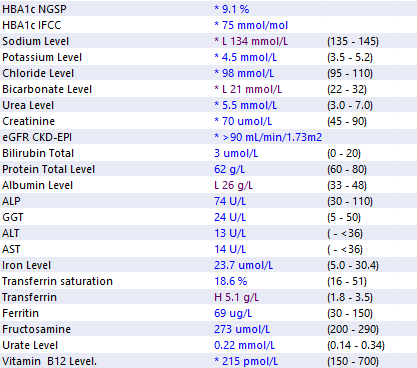
Intepret these results and what changes you make to your overall plan, if any?
Reassuringly, her FBC, electrolytes, renal function and iron studies are normal. Of greatest concern is her severely raised HBA1c. I would check her random BSL now to screen for hyperglycaemia and refer her to an Endocrinologist if Obstetrics haven't already done so.
{She is referred to an Endocrinologist who struggles to control Olivia's labile BSLs)
Explain how you assess and manage her suxamethonium and morphine allergies?
Clarify when allergies occured, the clinical context and the actual reaction. Reaction to sux can be one of several life threatening conditions: anaphylaxis, suxamethonium apnoea, malignant hyperthermia. Critical to obtain any allergy test results, especially for suxamethonium For morphine, alternative opioids can easily be used - however it may mean omitting it from a potential neuraxial block which could jeopardise high quality analgesia. Management: avoid the drugs - with the caveat that a CI to suxamethonium may also mean CI for other anaesthetic drugs depending on the cause.
Her reaction to suxamethonium happened when she was 4 years old. There are differing reports and remains unclear if she had anaphylaxis or sux apnoea. There has been no formal testing. She gets severe itchy rash from morphine and wants to avoid it. How do these ADRs impact your anaesthetic plan?
Any intra-operative anaesthesia and post-op analgesia will require modification. There is at least a 10% crossover of anaphylaxis between suxamethonium and rocuronium. I would carefully review old anaesthetic records to determine which NMB has been safe for Olivia and use the same. If it remains unclear, in the setting of a GA I would perform a modified RSI with atracurium, remifentanil, propofol and a topicalised larynx to minimise the risk of anaphylaxis and aspiration. (there can be several different alternative strategies to RSI and intubation without using sux and roc). For a neuraxial block I would avoid morphine altogether. For post-op analgesia, I would optimise multi-modal analgesia with USG bilateral TAP blocks, prescribe an oxycodone PCA for the first 24h and regular paracetamol and diclofenac (any NSAID is acceptable, including intra-op parecoxib).
Given her history of a difficult epidural and scoliosis, your anaesthetic registrar performs a point-of-care lumbar spine ultrasound. Outline the key landmarks in this image and where you would target the tip of your Touhy needle for a labour epidural? (click here to reveal image)
[labelled US image]
This is an transverse view of the lumbar interspinous space…
CHALLENGE QUESTIONS
At 35 weeks gestation, Olivia presents to the Pregnancy Day Stay Unit with a persistent dull throbbing headache. You have just finished your pre-admission clinic in the adjacent room and as you make an exit the Obstetric JMO requests your help. She’s concerned about Olivia’s blood pressure reading 168/100 mmHg. Her registrar is busy with a instrumental delivery and she’s not sure what to do. How do you help her?
Candidate should demonstrate a systematic list of differentials and a corresponding assessment and management approach. Avoid fixating on certain diagnoses and overcalling the situation.
Promptly assess Olivia with focused history, exam and consider investigations.
Advise transfer to birth unit temporarily. Outpatient clinic is not the ideal place for managing this.
Likely migraine given her history of increased frequency during pregnancy.
Cautiously rule out more serious or life threatening causes including:
- Pre-clampsia
- Intracranial haemorrhage / stroke
- Central vein thrombosis
- Severe hypo/hyper-glycaemia
- HONK
You make a provisional diagnosis of pre-eclampsia. What is severe pre-eclampsia? What is the risk of untreated hypertension?
Severe pre-eclampsia:
SBP>160 mmHg, DBP >110 mmHg with signs of organ dysyfunction e.g. proteinuria, AKI, liver dysfunction, neurological complications such as seizures, or haemtological abnormalities including thrombocytopaenia after 20 weeks gestation, and resolves within 3 months post-partum.
Risks / Complications
CVS
- Hypertension SBP>140mmhg, DBP >90mmhg
- Decreased intravascular volume (peripheral oedema)
- LV failure
NEURO
- Hyperreflexia
- Clonus
- Headaches
- Visual changes: photopsia, scotomata, papilloedema
- Confusion
- Seizures (eclampsia)
- If severe and uncontrolled-> intracerebral haemorrhage / stroke
RESP
- Pulmonary oedema
- Airway oedema
RENAL
- Proteinuria
- AKI
- Increased uric acid (decreased clearance)
HAEM
- Thrombocytopenia
- Coagulation dysfunction
- HELLP syndrome progression
FOETAL
- IUGR
- Placental abruption
- Unplanned preterm birth
- Foetal death
Describe your management of her blood pressure
Sit patient up
Repeat all vital signs. Telemetry monitoring and 5 minutely BPs until improving
IV access
Hydralazine 5 - 10mg IV, repeat every 20min
Other drug options: SNP 0.25mcg/kg/min or GTN 10mcg/min (must recognise this is last resort option and requires advanced monitoring)
Continuous CTG monitoring for foetal well-being
If Labetalol is offered the candidate must follow-up with the caveats and need for caution (not contra-indication) in the setting of existing CCB therapy (verapamil) and the risk of bradyarrhythmia including CHB and excessive negative inotropy. Prompt candidate if this reasoning is omitted.
Once stabilised increase Verapamil SR (e.g. double to 180mg BD)
Alternatively: add Nifedipine SR 20 - 60mg (oral) or Methyldopa 250mg - 750mg TDS for maintenance when stabilised
Contact Obstetrician recommending admission for further observation and treatment and workup for pre-eclampsia.
If remains refractory start hydralazine infusion to temporise and consult Obstetrician regarding emergency Caesarean Section.
How quickly would you reduce her hypertension?
5 – 10mmHg per 5 – 10 minutes aiming for < 150/100 mmHg. This minimises the risk of placento-foetal hypoperfusion (maternally dependent. No autoregulation)
Olivia’s headache resolves with your treatment. However, she has persistent scotomata, RUQ pain and hyperreflexia. There is oedema up to her mid-thighs. A urinary protein/creatinine ratio is 134 mg/mmol. Her blood pressure is now 155/90 mmHg after a total of 20mg IV hydralazine. What else will you do?
Other antihypertensive agents / infusions may be mentioned. But the crux at this point, is the consideration of Magnesium Sulphate infusion to prevent eclampsia and volunteer the loading dose, maintenance dosing and monitoring required. Otherwise prompt candidate.
- 4g IV over 20min (premix bag of 100mL) then 1g/h (i.e. 25mL) - reduces risk of convulsions by 50% (MAGPIE Trial
- Severe pre-eclampsia may cause renal impairment. If UO < 20mL/h and Cr > 200 umol/L increased risk of magnesium toxicity - strongly consider withholding maintenance infusion or reduced dose. Will need obstetrician consultation in this situation.
- Monitor for clinical symptoms of toxicity and increased frequency of standard observations
- Serum Mg2+ levels are should not be routinely checked but on suspicion / risk of toxicity
If the candidate specifically volunteers NOT to give Magnesium Sulphate then they must be prompted to give a rationale.
Valid arguments include:
- symptoms of pre-eclampsia have poor predictability for eclampsia
- at 35 weeks gestation and aiming to delay delivery till 37 weeks, when would the infusion cease after starting it now? A prolonged MgSO4 infusion > 5 - 7 days risks maternal side effects and foetal maldevelopment (skeletal effects, hypocalcaemia and hypermagnesemia)
- does not guarantee complete seizure prophylaxis. NNT = 50 (MAGPIE Trial).
- MgSO4 does not prevent progression of the underlying disease process of pre-eclampsia
The obstetrician agrees with the diagnosis of pre-eclampsia. She’s admitted to the birth unit for close observation. You are on-call that night and at 2:00am the obstetrician requests you promptly return in view of a possible emergency LSCS for Olivia. She has developed a bradycardia. How do you assess her when you arrive?
ABCD approach
- BP, HR
- ECG
- recent bloods: UEC, CMP
- review medications, especially antihypertensives (any beta-blockers, CCB?)
Likely differentials:
- Reflex bradycardia from severe hypertension of pre-eclampsia
- Antiarrhythmic / negative chronotropic effect from antihypertensives (more so with IV boluses or infusions)
- MgSO4 toxicity
- De novo bradyarrhythmia: AV block, prolonged QT
On examination, Olivia appears drowsy but rousable. Her speech slurred and her previous hyperreflexia has resolved. Her vision has less black spots but now blurrier than before. The new medications since admission include IV MgSO4 infusion 1g/h, labetalol 100mg TDS, verapamil 180mg BD.
BP 145/92
HR 47
SpO2 96% RA
RR 8
How do these findings influence your assessment and management?
MgSO4 toxicity more likely. Excessive beta-blockade may cause some of these symptoms.
A serum Mg2+ would give a definitive answer
Would not delay treatment while waiting for the result.
Temporise in interim:
- Cease magnesium infusion
- Calcium gluconate 10mL 2.2mmol or calcium chloride 10% (1g in 10mL) over 10min
- Serial ECGs and clinical examination
- Check CTG and foetal well-being
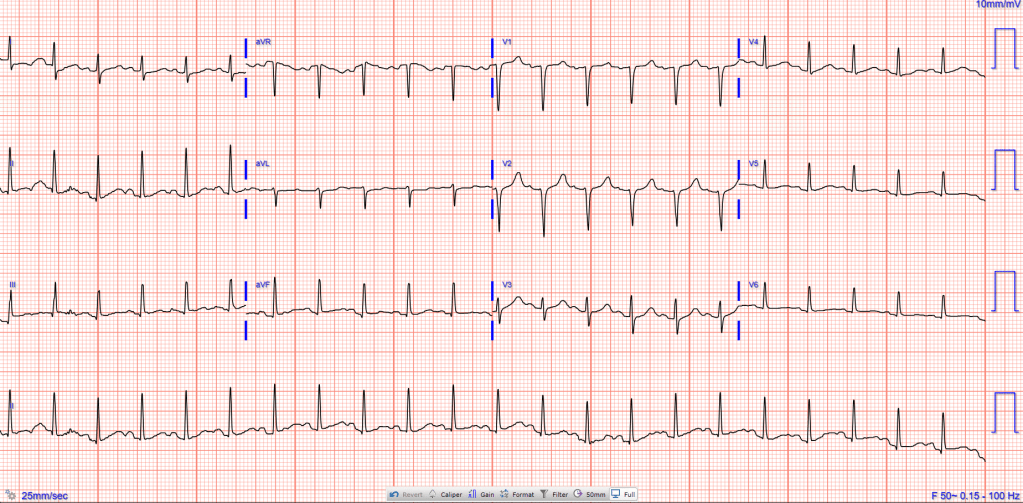
Interpret this ECG
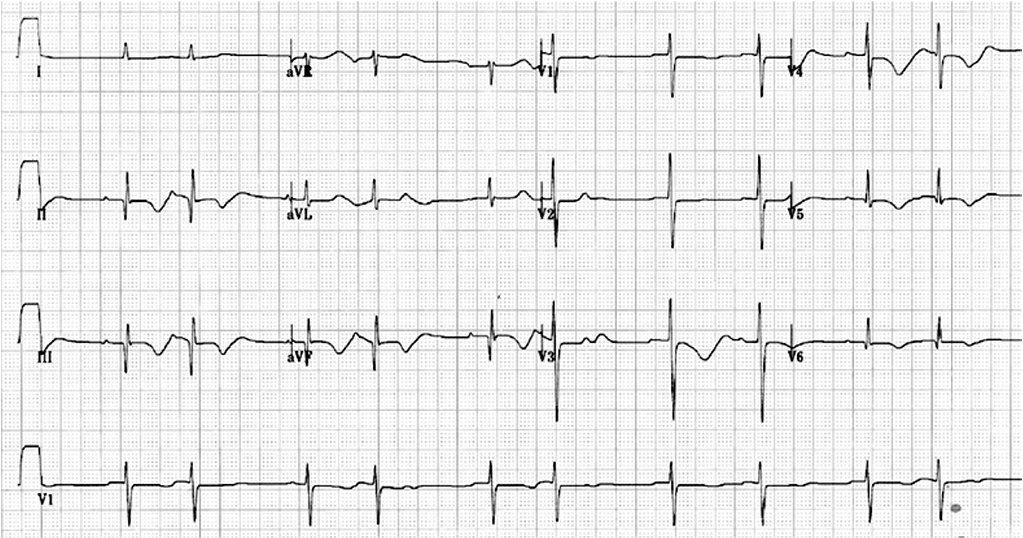
1st degree AVB (PR interval 218 msec), HR 30
Prolonged QT interval (corrected QT: 545 msec)
Atrial bigeminy
T wave inversion (II, III, aVF, and V4-6 lead) , and first degree atrioventricular block
What is the normal range for serum magnesium? What is considered toxicity when receiving an infusion for preventing eclampsia?
Normal 0.7 - 1.0 mmol/L
Toxicity is > 4.0 mmol/L
She has good response to the treatment and her toxicity symptoms gradually resolve.
Fast forward to 37 weeks gestation, it is now day of surgery for Olivia’s LSCS. Hypertension has been well-controlled in the last week. Her platelet count has been steadily dropping however, with yesterday’s count at 72 x 109/L. Explain how you’ll proceed with your anaesthetic?
Neuraxial technique is preferred.
Need updated platelet count, within last 6h and a review of coagulation profile.
Delay surgery until count known
Hard threshold (e.g. 70 x 109/L), assuming no coagulopathy
(Candidate can have a different threshold)
Her LSCS is postponed to second on the list, pending FBC. It returns with a platelet count of 80 x 109/L. Your registrar proceeds with a CSE under your instruction. As the spinal block dose is injected, the syringe dislodges and the remainder squirts out forcibly onto the sterile drape. How do you manage this situation?
A sensible response is all that is required. e.g.:
- open disclosure to patient
- maintain patient safety: continue monitoring vital signs, check for any onset of paraesthesia i.e. some spinal anaesthetic was administerd), instruct the trainee to maintain a fixed standy hand on Touhy and spinal needles
- inspect for continuous steady drip of CSF to confirm subarachnoid position of spinal needle
- Put on sterile gown and assist trainee to re-prepare spinal anaesthetic drugs, using a Luer-lock syringe to avoid chance of slipping syringe in second attempt
Alternative options:
a) trainee aborts completely, prepares drugs again and re-attempts
b) you take-over as primary proceduralist and trainee draws up new drugs
c) abandon spinal and use epidural only - least practical option but feasible. If candidate has this response prompt how they would do top-up and rationale for this approach
Inappropriate options:
a) letting go of neuraxial needles to draw up drugs again (potentially unsafe, could lose critical subarachnoid / epidural space if patient moves, consultant is in the room why not ask for help?)
b) requesting the anaesthetic nurse (unsterile personnel) to draw up drugs again
c) over-calling the challenge by hitting emergency button (causing unnecessary panic, diverting resources inappropriately)
The CSE is salvaged, Olivia has an appropriate block to T5 and the Caesarean section proceeds. You leave the patient in your trainee’s care and break for lunch in the tea room. When you return the nurse anxiously says “oh just in time. I was about to call you. The patient is struggling to breath.” You see your trainee behind her gathering airway equipment. How do you assess this situation?
Requires a systematic approach and demonstration of situational awareness
Assess patient's ABCD including her vital signs for any life-threatening observations
Communicate the problem to the surgeon and determine the stage of surgery. Has the neonate has been delivered?
Obtain a rapid handover from trainee, sequence of events and treatment so far
Further history and examination of the patient including associated:
- pain, dyspnoea, coughing, vomiting, aspiration, upcreeping paraesthesia affecting arms or face
And signs of:
- increased WOB, crackles/creps on auscultation, coughing secretions / sputum
What are you differentials at this point?
- Inadequate spinal block -> pain (complicated block with extra handling and time with needle spent insitu. May have moved)
- High spinal block (partial dose from first spinal syringe was given)
- Aspiration
- Asthma flare
- Emoblism: PE / AFE
- Anaphylaxis
- Panic attack
Your registrar reports Olivia had a post-partum haemorrhage of 1.5L and tachycardia up to 120 bpm. In response, 3L of 0.9% sodium chloride was bolused, 10 units of syntocinon STAT and 250mL/h infusion of syntocinon (10 units/h) was started. She started complaining of dyspnoea shortly after this. On auscultation she has bibasal inspiratory creps. How does this influence your differential diagnosis and what is your management?
This patient has severe pre-eclampsia with impaired renal function and peripheral oedema at baseline.
She is more susceptible to fluid overload and she now has APO secondary to aggressive crystalloid fluid resuscitation. Likely worsened with large dose syntocinon followed by a large volume infusion.
Priorities of management:
- optimise gas exchange
- restrict fluid administration to prevent overload
Supplementary O2
Communicate events to surgeon and question if bleeding and uterine atony still problematic
Inform and reassure patient
Reverse Trendelenberg position to improve FRC and reduce atelectasis
IV furosemide (e.g. 20 - 40mg) provided no hypotension
- alternatively / additionally give GTN 25 - 50mcg
Replace IV syntocinon infusion with a more concentrated one e.g. 40 units in 500mL (0.08 units/mL). If targeting 10 units/h = 125mL/h
Avoid any further IV fluids
Instead, PRBC and TXA 15mg/kg if any further bleeding
Be prepared to escalate to HFNO or NIV if SpO2 falls
CXR in PACU
Notify HDU/ICU for post-op admission
AFTERMATH QUESTIONS
Olivia has a 300mL diuresis. By the end of the surgery, her dyspnoea improves slightly. A mobile CXR in PACU shows pulmonary oedema. NIV is started, she is transferred to HDU and recovers well. A few days later you hear other trainees gossiping about your registrar actions, resulting in an obstetric patient requiring intubation for APO. How do you handle this situation?
Key issues
- Professionalism
- Well-being of junior colleagues
Gossip undermines trust and learning. This situation suggests misinformation and there's a risk of psychological harm to my registrar.
Address these trainees privately and promptly. Clarify what they believe has happened and correct the events.
Remind them of their responsibilities to act professionally with respect and confidentiality.
Seek out my registrar and facilitate a private, non-judgmental debrief session.
Show empathy and allow the registrar to drive the discussion, which enhances their own reflective practice and learning.
Offer the opportunity to use this as a WBA e.g. CbD and provide actionable feedback e.g. podcasts / review articles for managing severe pre-eclampsia.
END OF VIVA
Sources
Satya Francis, Anne May, Pregnant women with significant medical conditions: anaesthetic implications, Continuing Education in Anaesthesia Critical Care & Pain, Volume 4, Issue 3, June 2004, Pages 95–97, https://doi.org/10.1093/bjaceaccp/mkh026
NICE Guidelines on hypertension in pregnancy 2023
D Leslie, RE Collis, Hypertension in pregnancy, BJA Education, Volume 16, Issue 1, January 2016, Pages 33–37, https://doi.org/10.1093/bjaceaccp/mkv020
Guideline for the Management of Hypertensive Disorders of Pregnancy SOMANZ, 2014.
D Leslie, RE Collis, Hypertension in pregnancy, BJA Education, Volume 16, Issue 1, January 2016, Pages 33–37, https://doi.org/10.1093/bjaceaccp/mkv020.
Royal Hospital for Women (RHW) CLINICAL BUSINESS RULE: Magnesium Sulphate for Eclampsia or Eclampsia Prophylaxis. April 2023.
Bauer ME et al. The Society for Obstetric Anesthesia and Perinatology Interdisciplinary Consensus Statement on Neuraxial Procedures in Obstetric Patients With Thrombocytopenia. Anesth Analg. 2021 Jun 1;132(6):1531-1544. doi: 10.1213/ANE.0000000000005355. PMID: 33861047.
