Carol is a 31 year old pregnant woman planning a natural birth. She has been referred for consultation about epidural analgesia. She has developed a foot drop since 25 weeks pregnant. A MRI spine and nerve conduction studies of the leg did not identify a cause.
Past Medical History
Asthma
Current Medications
Nil
Allergies
Nil
OPENING QUESTION
Candidate has 2 minutes reading time to plan their initial response to the first question below
Click each question to reveal a suggested answer
Describe your initial assessment?
Candidates should give a short opening statement signposting the concerning features of this obstetric patient, followed by an overview of the assessment in focused history, exam and review of relevant investigations.
At minimum, the following features should be specified:
History
Obstetric: gestation, previous pregnancies and anaesthetic modalities
Foetal: growth issues, abnormal placental implantations
General: diabetes, obesity, cardiorespiratory, severity of asthma
Specific to foot drop:
pre-existing neurological diseases
trauma to leg/foot/spine
CNS symptoms: headache, visual disturbances, vertigo, balance/coordination issues, CSF leak
Examination
Vital signs
General neurological exam, including CN exam, inspection of gait and specifically exam affected leg/foot
Cardiorespiratory exam
Airway assessment
Investigations
Review MRI spine and NCS reports
Review correspondence from neurologist
PROGRESS QUESTIONS
Carol is G1P0, now 37 weeks gestation. She denies any other medical history apart from asthma during childhood. There was no trauma or injury related to her left foot drop. No associated headaches or changes in vision.
She noticed it during second trimester and it has been gradually getting worse, with some weak knee extension now too. It’s more noticeable when she uses stairs. She uses an orthotic splint for her left foot to walk properly.
She asks you if an epidural will make this problem worse. How do you manage the remainder of this consultation?
The candidate needs to demonstrate a holistic approach to the patient and prioritise seeking a diagnosis for Carol's focal neurological deficit. This problem needs further specialist consultation and investigation. It is completely abnormal for a well pregnant woman to suddenly develop a foot drop.
Reinforce concerns of a serious neurological problem especially given the progression of symptoms.
Recommend an urgent MRI-B and Neurosurgical consultation
A CT-Brain is urgently booked 2 days later. (Click to open images)


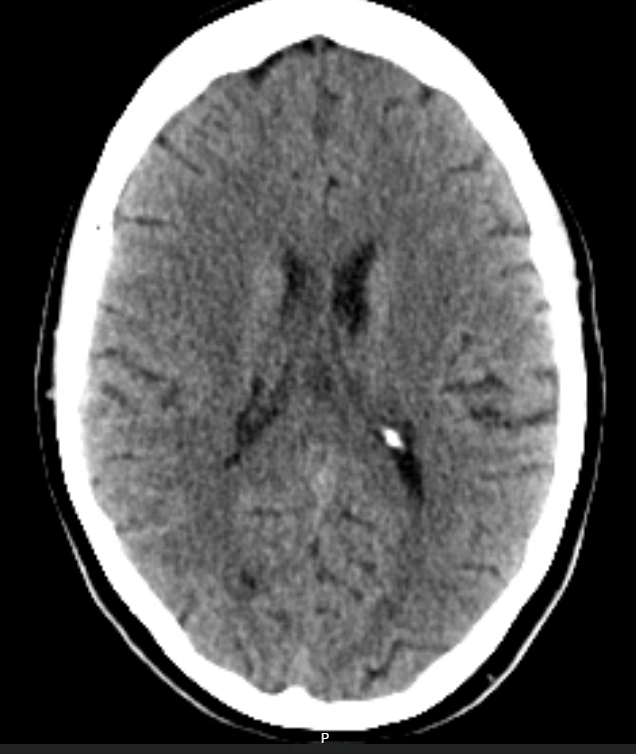
Describe these CT images
Axial slices
Large hypodense space-occupying lesion in the right frontal/pareital lobe
Poorly defined borders
Midline sulcal effacement and minor midline shift
No ventricular obstruction
No obvious signs of raised ICP
CHALLENGE QUESTIONS
Carol is seen by a Neurosurgeon who diagnoses her with a form of glioma. Surgical resection is recommended but not urgent. Her neurosurgeon will plan for a craniectomy when Carol has well recovered from her postpartum period.
Now at 38 weeks gestation she returns to your anaesthetic clinic. What are the peripartum anaesthetic concerns?
1. Safety of neuraxial anaesthesia This is a key decision point. Pros of Neuraxial Analgesia: - Attenuates stress response and ICP surges from pain and bearing down during labour - Allows titration and flexibility (e.g., extend for emergency LSCS). - Promotes more stable haemodynamic profile. Risks: Spinal or epidural anaesthesia could be hazardous if: - Glioma extends to spinal cord or causes CSF flow obstruction. - There is risk of herniation from dural puncture (though low without raised ICP). - Neurological deficits complicate post-procedure assessments (distinguishing pre-existing weakness vs new deficit). Strategy: Imaging review is critical (ideally brain and spine MRI) to rule out raised ICP Ensure pre-existing stable deficits are documented Epidural catheter is acceptable and arguably the safest Avoid spinal block due to unpredictable CSF pressure gradients and potential for brain herniation Alert anaesthetic department when patient is admitted for IOL Procedure by Consultant Anaesthetist only 2. ICP Considerations Current imaging is reassuring, however ICP can change rapidly with tumour progression and physiological changes in pregnancy, especially in labour: - Labour pain and Valsalva during second stage can increase ICP via increased intrathoracic and venous pressures -> therefore early epidural prior to induction of labour (IOL) provides greatest control. - Care with EDB if space-occupying lesion evolves, as the extra bolus of fluid against a pressurised dura may exacerbate raised ICP and compromise CPP. - these concerns extend to a GA for emLSCS, particularly during laryngoscopy, intubation, delivery of foetus and tracheal extubation - alternatively an elective LSCS under EDB Top-up is also a safe valid alternative 3. Neurological Observations Should be incorporated with standard obstetric observations during labour and post-partum. Via MDT with Neurosurgery, discuss possibility of neurological deterioration post-procedure due to either disease or anaesthesia-related factors. Deliver in a tertiary centre with Neurosurgical support 4. Anaesthetic Considerations for Emergency LSCS a) EDB Top-up b) If GA required: - Avoid agents that increase ICP (e.g. ketamine, high-dose volatile agents). - Use RSI with attention to ICP-neutral techniques: e.g. Lidocaine, remifentanil, labetalol Ensure mild hyperventilation only (ETCO₂ 30-35 mmHg). Facilitate cerebral venous drainage: elevate head, tape not tie ETT.
Discussion around the risk of brain herniation, although relatively low, has made Carol very anxious. She prefers to avoid an epidural and see how she fairs without it. What other analgesic modalities are suitable?
Candidate should have a systematic approach. e.g. pharmacological vs non-pharmacological.
Remifentanil PCA must be included.
Level of evidence should be stated. Prompt if required - "which has best evidence?"
Pharmacological
N2O
Opioids (IM/SC/PO)
*Remifentanil PCA
Non-Pharmacological
*Continuous presence of trained support person
Mindfulness / meditation
Hypnosis
TENS
Massage
*Water bath / immersion / hydrotherapy
*Acupuncture
Aromatherapy
'Waterblocks' / SC water injections in back
*there is Level 1 / 2 evidence for these options in providing the most efficacious analgesia and/or greater maternal satisfaction
Explain how you would safely set up a remifentanil PCA for labour?
A standardised protocol for the specific institution must be followed and midwife must be trained in managing PCA devices.
In the absence of a protocol, the midwifery team specifically for this patient must be comfortable in following the strict clear written instructions from me. Otherwise for patient safety, the PCA should be abandoned for other alternative analgesia modalities.
Drug Preparation
Concentration: 20mcg/mL (e.g. 2mg in 100mL)
Bolus: 20 - 40mcg (1 - 2mL)
Lockout: 3min
No background infusion
Patient Preparation
IV access
Supp O2
Informed consent and understanding of PCA system
Monitoring
Increased vital sign monitoring:
- BP 30 minutely
- RR + sedation score 15 minutely
- Continuous SpO2 and ideally capnography
Rescue Protocols
Standing order for naloxone if oxygen desaturation < 94% or sedation score >/= 2
Thresholds for initiating urgent clinical review and anaesthetic review
You are on-call for obstetric anaesthesia. At night you receive a call from birthing suite. Carol has come in for her IOL and has been using a remifentanil PCA to manage her contraction pain. The midwife is very concerned about drowsiness and low respiratory rate. How do you respond to this call?
Candidates may be tempted to tunnel vision onto the remifentanil PCA. While correct, a strong answer should demonstrate a systematic approach, to avoid missing less likely but dangerous causes, particularly in this specific patient.
Attend to the call.
Primary differentials:
- Opioid toxicity from Remi PCA
- Intracranial event (incl haemorrhagic or ischaemic stroke)
- Epilepsy secondary to known brain tumour
While enroute:
Immediately instruct the midwife to activate an urgent clinical review by a medical officer
Ask for vital signs including GCS and if PEARL.
Ask for any compromise to foetus e.g. foetal brady / abnormal CTG
Instruct staff to:
- continually monitor maternal vital signs
- Support airway with chin lift / jaw thrust to prevent obstruction
- Apply supplementary O2 e.g. NRB mask
On arrival get rapid handover from staff, reassess ABCD, particular focus on GCS, pupils and and focal neurological deficit.
Review the set up the of remifentanil PCA, to rule out drug related causes and consider nalaxone if concerned about opioid toxicity.
On arrival. Vital signs: BP 98/70, HR 63, RR 7, SpO2 93% on 15L NRB mask. GCS 14. PEARL. Midwife reports initially some foetal brady but improved with left lateral positioning and applying oxygen. The JMO is supporting the patient’s airway with a chin lift. You review the PCA setup (click this question to reveal) and notice this:
Volume 90mL. Running.
Remifentanil 40mcg/mL
Continuous rate: 0
PCA Dose: 2mL
PCA Lockout: 3min
Interpret these settings. Describe your management of the patient now
PCA has been incorrectly setup. Bolus dose is double the standard and for an opioid naive patient, this can result in opioid overdose - which is most likely the reason for Carol's respiratory depression.
Naloxone 100mcg STAT and repeat another 4 times as required every 2 minutes and assess for response.
If her sedation continues to rebound I'll start an naloxone infusion. She'll then need to be transferred to HDU. In this setting, I would consult the Obstetric team regarding her delivery plan and the timing. It would be prudent to correct the opioid toxicity first prior to any expedited LSCS in case the foetus is narcotised.
If she has no response to naloxone this is extremely concerning for an intracranial event and an urgent CTB is required with Neurosurgical and Obstetric consultation.
AFTERMATH QUESTIONS
Carol responds to 2 doses of Naloxone and maintains consciousness. There is no neurological deficit and she is weaned off the oxygen. CTG has remained normal. The obstetric team are keen to continue her syntocinon infusion and her labour. They ask about her analgesic options. What is your plan?
Recommend an epidural
+/- USS spine first to gauge expected depth of ligamentum flavum and posterior complex to reduce risk of dural puncture.
END OF VIVA
Sources
G Lim, AM Bader. Chapter 48 Neurologic and Neuromuscular Disease, Chestnut's Obstetric Anesthesia 6th Edition 202, Pages 1160-1189.
KK Lam, MKM Leung, MG Irwin. Labour analgesia: update and literature review. Hong Kong Med J 2020;26:413–20 https://doi.org/10.12809/hkmj208632.
Caroline Fortescue, Michael YK Wee, Analgesia in labour: non-regional techniques, Continuing Education in Anaesthesia Critical Care & Pain, Volume 5, Issue 1, February 2005, Pages 9–13, https://doi.org/10.1093/bjaceaccp/mki002.
The Royal Hospital for Women. PATIENT CONTROLLED ANALGESIA (PCA) REMIFENTANIL – IN LABOUR, LOCAL OPERATING PROCEDURE - CLINICAL. May 2021.
